Estimated Results
HBES primarily aimed to design, deliver and evaluate a novel assistive and rehabilitation device for people with upper limb disabilities, e.g. related to stroke, spinal cord injury (SCI) and brain injury, leading them to a better life and social integration. Research included: modelling of the mechanical structure and of the Functional ELectrical Stimulation (FES) system and development of hardware and software platforms for exoskeleton and BCI.
HBES system configuration
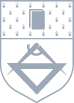
The first stage of the project aimed to configure the HBES system in terms of sketches developed based on a bibliographic study. Thus, the upper limb biomechanics was investigated, in order to develop the arm cinematic model.
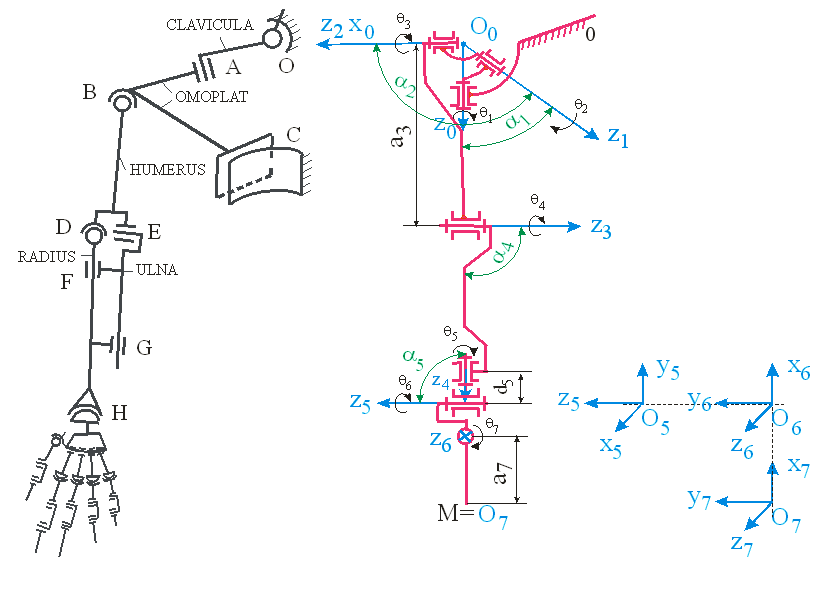
The research also aimed at identifying technical solutions for developing the rehabilitation system for the human upper limb. In parallel, the modeling, analysis and synthesis of the FES system was carried out, identifying the positions where the FES electrodes can be placed in order to induce the movements necessary for the arm rehabilitation process as specified by the medical staff.
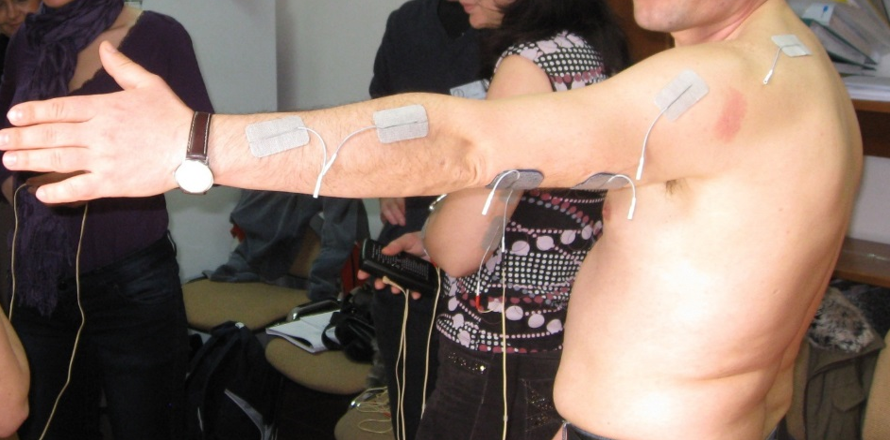
The control block diagram of the HBES prototype is presented in the following figure. The BCI system records the EEG signals and transmits them to the coordinating computer that performs the signal processing, feature extraction and classification. It transmits then the results to the exoskeleton and FES unit coordinating computer. Based on the received results, it coordinates both the stimulation parameters of the FES unit and the movements of the exoskeleton joints. These movements are transmitted to the server microcontroller (Server MCU), which gives the reference signals to the motor regulators (PID MCU & controller), and transmits back to the coordinating computer the positions, angular velocities, etc. of each joint.

For the integration of the hardware and software components, two computers were used, due to the fact that both, the algorithm for processing and interpreting the data for the BCI system, as well as the applications for the exoskeleton and the FES system control, require very high computing power. Communication between the software subsystems on the two computers is done via the TCP/IP interface. The following figure schematically shows the working principle of the HBES prototype.
The BCI system reads the EEG signals, preprocesses them locally, and sends them to the computer where the algorithm for processing and classifying the BCI signals was implemented. After extracting the user's intention, a command is transmitted via TCP/IP to the computer that controls the exoskeleton and the neurostimulator to achieve balanced control between the FES and the movements of the exoskeleton's joints. All software applications were developed in the Matlab&Simulink programming environment.
Laboratory tests
During the laboratory tests, different forward-backward projection of the arm and flexion-extension of the elbow joint were designed. During the entire duration of the exercises, the M1 motor, which performs adduction/abduction of the shoulder, was programmed to maintain an angle of 15 degrees to the vertical axis, according to the following figure.
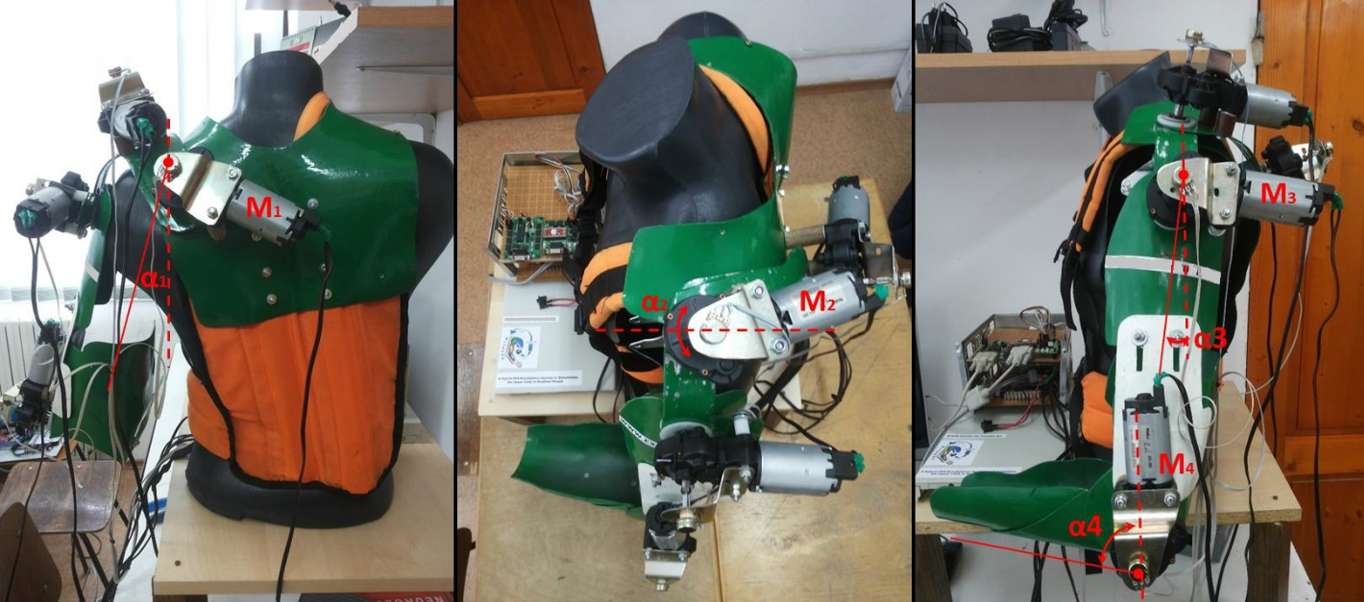
Motor M2, which performs the internal/external rotation movement of the shoulder was programmed to maintain the angle at zero degrees. Motor M3 performed forward-backward projection of the shoulder with α3 angle and motor M4 performed extension and flexion of the elbow with α4 angle. During testing on a healthy subject, channel 1 of the MOTIONSTIM8 neurostimulator was assigned to the M3 motor, with its corresponding electrodes placed on the triceps muscle in order to induce the elbow extension movement simultaneously with the M3 motor. Channel 2 of the neurostimulator was assigned to the M4 motor, and its corresponding electrodes were placed on the hand extensors, to induce the opening movement of the hand when the elbow joint reached the maximum angle prescribed for extension.
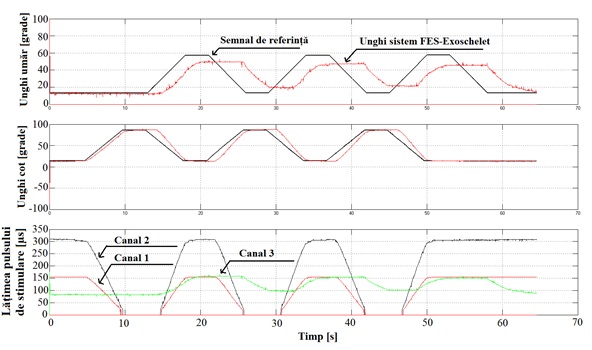
In order to perform flexion and extension movements of the paretic arm, FES was applied to the deltoid, triceps and hand extensors muscles. The stimulation channel - stimulated muscle correspondence was: channel1 - triceps, channel2 - hand extensors, channel3 - medial deltoid. The stimulation frequency was 50 Hz. Before starting the experiment, the maximum values of the stimulation signal parameters for each muscle group were tested, these values leading to the desired contraction for producing a functional movement. The following figure presents the reference signals, the positioning of the motors driving the shoulder and elbow joints, and also the stimulation signal pulse width variation for the three muscle groups mentioned previously.
Iterative improvement of the system
After conducting some preliminary tests with healthy subjects, we concluded that the introduction of the third class of motor imagery for the BCI system is also necessary. Consequently, an extension of the CSP method was implemented. Thus, we implemented the one versus all others CSP method. The user had to imagine the movement of the right hand versus the movement of the left hand or the movement of the legs, according to the clue presented by the paradigm. This algorithm was initially tested on 7 healthy subjects. The data used were processed similarly to the study carried out in the previous stage, resulting in a new method of choosing the parameters of the three-class motor imagery based BCI system.
Clinical tests of the HBES system
The main objective of the HBES project was to develop a hybrid BCI-exoskeleton-FES system for the recovery process of the upper limbs for stroke patients. In the last stage of the project, the system developed in the previous stages was tested in a clinical environment on patients with neuromotor deficit caused by stroke. Limited clinical trials included 10 patients with ischemic stroke. Patients were assessed using the arm component (parts I-VI) of the Fugl-Meyer scale, patient global impression of change (PGI-C), clinician global impression of change (CGI-C), and the Brunstromm scale. Clinical testing was performed before the start of the rehabilitation program and at its end, except for the PGI-C and CGI-C which were administered only after the training program. The impact of the rehabilitation program was favorable, with corresponding scores improvements on the Fugl-Meyer scale. There was a trend towards better improvement in practiced movements (subscale V), although quantitatively the increase in these components of the score was not sufficient to reach the significance threshold. The significant increase was generated by increases in all subscales. A direct impact on the movements practiced can thus be speculated, and potentially a wider improvement by increasing the type of movements included in the exercise program. With certainty, the magnitude of the changes is not sufficient to lead to a transition from one step to another on the Brunstromm scale. This scale, however, includes broad functional categories, and does not allow fineness evaluations of individual components. However, the functional importance of the improvements made by patients within the program remains to be determined.
Individually, the most important differences were found in patients with "average" damage within the group (score between 20 and 25), and less in patients with an initial score of 10-15 or in the patient with a score over 30. Of the 10 subjects , 4 did not register an improvement in the Fugl-Meyer score, 2 registered an increase of 1 and 2 points respectively, one subject registered an increase of 3 points, the maximum difference (of 5 points) being recorded in only one case . It is possible that, given the small number of subjects, individual growth significantly influences the statistical results, but significance is preserved even if the subject with the largest growth (5 points) is excluded (p=0.028).
Publications
Dissemination of the project results was achieved through:
- Publications in journals with impact factor:
Hayta, Ünal, Danut Constantin Irimia, Christoph Guger, İbrahim Erkutlu, and İbrahim Halil Güzelbey. 2022. "Optimizing Motor Imagery Parameters for Robotic Arm Control by Brain-Computer Interface" Brain Sciences 12, no. 7: 833. https://doi.org/10.3390/brainsci12070833, Impact Factor: 3,333.- Publication in ISI WOS & BDI indexed conference volumes:
Mitocaru A., Poboroniuc M.S., Irimia D.C., Baciu A.G., Comparison between two Brain-Computer Interface systems aiming to control a mobile robot, 2021 International Conference on Electromechanical and Energy Systems (SIELMEN), 6-8 Oct. 2021, Iasi, Romania, DOI: 10.1109/SIELMEN53755.2021.9600389, indexed IEEE Xplore.
Marian Poboroniuc, Danuţ Irimia, Radu Ionaşcu, Andrei Iulian Roman, Alexandru Mitocaru, Alina Baciu, Design and Experimental Results of New Devices forUpper Limb Rehabilitation in Stroke, The 9th IEEE International Conference on E-Health and Bioengineering - EHB 2021, Grigore T. Popa University of Medicine and Pharmacy, Web Conference, Romania, November 18-19, 2021, IEEE 978-1-6654-4000-4/21/$31.00, indexed IEEE Xplore.
Ortner R., Dinarès-Ferran J., Irimia DC., Guger C. (2021) Towards Improved Vibro-Tactile P300 BCIs. In: Kurosu M. (eds) Human-Computer Interaction. Interaction Techniques and Novel Applications. HCII 2021. Lecture Notes in Computer Science, vol 12763. Springer, Cham. https://doi.org/10.1007/978-3-030-78465-2_6.
Participation to Inovation expositions:
Participation at EUROINVENT Outstanding Innovation Expo 2022, with HBES prototype under the name: Brain-Computer Interface to control a humanoid/mechanical robot. The HBES system was awarded with the Gold Medal.